A project to improve care for patients with complex conditions, who are more likely to face barriers in following their doctors’ orders.
How can our healthcare community provide equitable care for complex patients?
The Story
Hennepin County Medical Center (HCMC) is a safety net hospital in Minneapolis, MN with a system of primary care clinics and retail clinics that provides care for populations that are low-income, uninsured and vulnerable. For these “complex patients,” those defined by the combination of a chronic illness, a mental health condition and substance abuse, accessing the healthcare system poses difficulties that are often unseen and misunderstood. To better understand the people they serve, and support them in living healthier lives, HCMC used a human-centered design process for creative approaches.
HCMC engaged Greater Good Studio first, to conduct research and subsequently to help prioritize and prototype the best ideas that emerged from it. The project introduced a strategic shift towards a journey-based model of care, one in which health is viewed not as a destination or end goal, but as a practice of successfully moving a patient along on their journey.
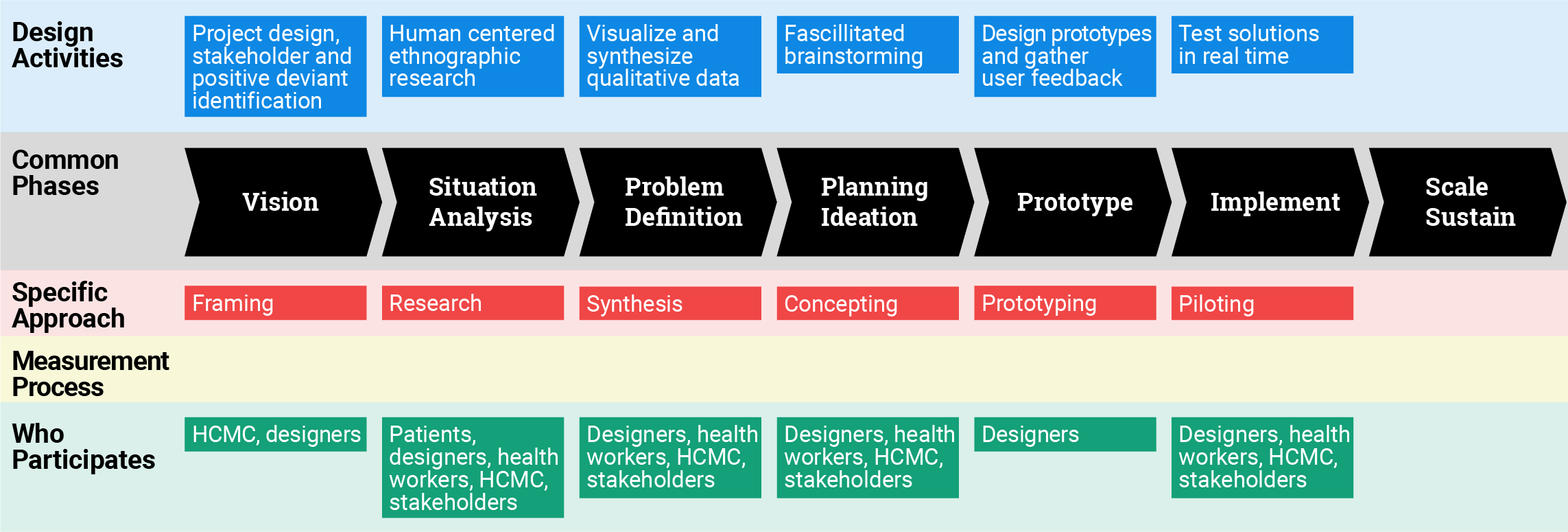
Process and Measurement
Amount of Design: End to End
The project began with initial one-on-one interviews with patients with co-morbid conditions — physical and mental health as well as substance abuse. The high level question driving this research was “why is our health care system not working for these patients?” Why do they so often not show up at the clinic and not follow doctor’s orders?
Patients were observed while they interacted with the healthcare system. On the day they had an appointment, designers met them at their home, traveled with them to the site. into the actual appointment when permitted, at other times not. Designers also traveled home with them after the appointment.
A second wave of exploration was to engage with HCMC’s large network of community partners in Minneapolis that serve the same population. Questions driving this research phase were “How are these organizations serving complex patients effectively?” “What can we learn about different ways to serve the same population?
Third phase of research was observation with a range of small but innovative program and service providers within HCMC. Designers spent time with people who were bridging the gap between patients and doctors, such as community paramedics and coordinated care clinics. They wanted to understand the full system of people who were serving these patients and working within or around system constraints.
Concept development was participatory. HCMC and Greater Good Studio hosted a large workshop to share research and develop ideas with many of the people who had been research participants. They wanted to “close the loop with people, to invite them to see what their contributions yielded.” Then, during a synthesis session with the client team, a large collection of ideas was narrowed to twenty. These concepts were shared with patients and providers, first via a survey and then via one-on-one prototype feedback sessions.
Over a period of four months, two concepts were piloted with support from Greater Good Studio. Another set of concepts were fast-tracked for implementation.
One example was co-created with Now-Pow, a social services platform that curates social services within a community, allowing community partners to more easily find resources for patients.
Another example is a self-service kiosk, placed in one of HCMC’s largest ambulatory settings. Because only 3% of patients are able to meet with community health or social workers, this is an effort to provide people with access to resources at the time they are needed.
Still another example is a transportation system whose purpose was to facilitate transportation to of clients to their appointments, reducing access barriers associated with lack of, unreliable transportation.
Greater Good Studio’s Process
Human-centered design is a problem-solving process grounded in empathy and iteration. It’s also a powerful framework for creating alignment among people from diverse backgrounds and turning ideas into action.
Framing
First, we design the project.
We don’t just create artifacts, we create engagements. Every project is intentionally designed to maximize ownership, implementation and impact by engaging end users at
We practice appreciative inquiry by positively framing projects in terms of solutions to achieve, rather than problems to fix.
We seek out positive deviants—the small number of folks who have created their own solutions—so we can learn from their work.
We find participants using the principles of relational recruiting, identifying key stakeholders and building partnerships with community-based organizations.
Research
Our learning happens in the real world.
Rather than surveys or focus groups, our research is about observing behavior in context. We believe that seeing and learning from people’s behaviors in real time is the best way to build empathy—the key to good design.
We take our interviews and exercises where our users are, so we can immerse ourselves in their realities.
We start by explaining our goals and purpose, so participants understand why we’re there and how important their role is.
We take a trauma-informed approach to working with vulnerable populations, building on strengths and creating an atmosphere of psychological safety.
Synthesis
We define opportunities around what is working.
Traditional design focuses on finding and meeting unmet needs, but we also focus on assets–the existing tools, habits and relationships we can support and scale through design.
We make our qualitative data tangible—filling the walls with photos, quotes and stories—to keep the team grounded in concrete examples.
We find themes and insights based on patterns of behavior, then make them generative with frameworks and “how might we” statements.
We share findings through compelling videos, engaging workshops and inspirational visuals that help teams take action.
Concepting
We use brainstorming as a tool for inclusion.
All brainstorms are not created equal. Our ideation sessions are facilitated to engage diverse stakeholders and bring out their creative confidence, so they can take an active role in designing their own solutions.
To keep brainstorms both focused and productive, we use thought-provoking tools such as user stories, “how might we” statements and solutions from analogous fields.
We defer judgment and go for quantity, so everyone can be comfortable sharing their insights.
We use storyboards to show how program and service ideas add up to a comprehensive experience.
Prototyping
We always prototype before we pilot.
Prototyping reduces the risk of trying something new. By finding fast, cheap ways to make our ideas tangible, we get closer to knowing what will work, what won’t and why.
Anything can be prototyped—from programs and services, to spaces, events and communications, as well as digital tools and products. We create props that simulate the full experience.
We gather user feedback so we can rapidly iterate on the prototype until it meets users’ needs.
By mimicking what the final product will really be like to use, prototypes are the best way to gather evidence instead of opinions.
Piloting
We test solutions in real time.
Piloting lowers the costs of implementing a new solution at scale. By testing our solutions at a small scale we can learn directly from users’ unbiased behaviors, while leaving space to address unanswered questions and new learnings that arise during each scale of implementation.
We plan pilots that make sense for our clients’ capacity, defining each specific element of implementation: what tasks need to be done, by whom, and on what timeline.
We determine the appropriate data to record and metrics to measure during our tests, recognizing that our definition of success might change with each piloting cycle.
Pilots include moments of reflection to refine solutions for the next scale of implementation.
The Role of Measurement
Greater Good Studio’s design process integrates several types of measurement, formal and informal. The team collects data using observation, individual discussion and feedback, and group discussion and feedback during the problem-framing phase. They employ standard data collection tools but “leave space to address unanswered questions and new learnings that arise during each scale of implementation.” The flexibility afforded in any measurement strategy is key at this stage of the design process. As noted by a GGS team member, “we determine the appropriate data to record and metrics to measure during our tests, recognizing that our definition of success might change with each piloting cycle.”
For prototyping solutions, GGS define around five short-term goals to guide decision-making and solution iteration. These goals are later expressed as decision metrics related to, for example, improved patient experience. Metrics such as interest, comfort, confidence and preference determine the extent to which the prototype is becoming increasingly acceptable to users. They also frame five or so long-term goals that they use to assess the effectiveness of the intervention once it enters the implementation phase possibly a pilot rather than full-scale implementation. This two-stage goal (and metric) framing is akin to a theory of change pathways used in program strategy development and evaluation, where long-term changes are reliant on meeting specific pre-conditions (short-term changes) and interventions are assessed according to their ability to bring about those preconditions. At one time, the GGS team surveyed key stakeholders to prioritize a short-list of solutions, hoping to move from 15 ideas to a more limited number that could then be prototyped. However, they concluded that this kind of ranking of yet untested/unprototyped ideas was not an effective measurement approach for either the client or the design/intervention team. (See complete concept feedback survey results.)
In terms of evaluation of the programs generated through the design process, for Hitch Health, an assessment of the 12-month pilot at the Hennepin Healthcare internal clinic captured three metrics: the “client no show” rate (27% reduction), estimated change in clinic revenue ($270,000 increase), both of which were used to calculate a return on investment (ROI) of 297%. The simple assessment documented that the intervention was beneficial to clients (who accessed services more easily and consistently) and the service delivery organization that reduced costs. There was no deliberate evaluation of the link between a social design process and social outcomes. However, GGS and their client both reported that the design process facilitated a more effective partnering and deepened partnerships between HCMC and their community collaborators.
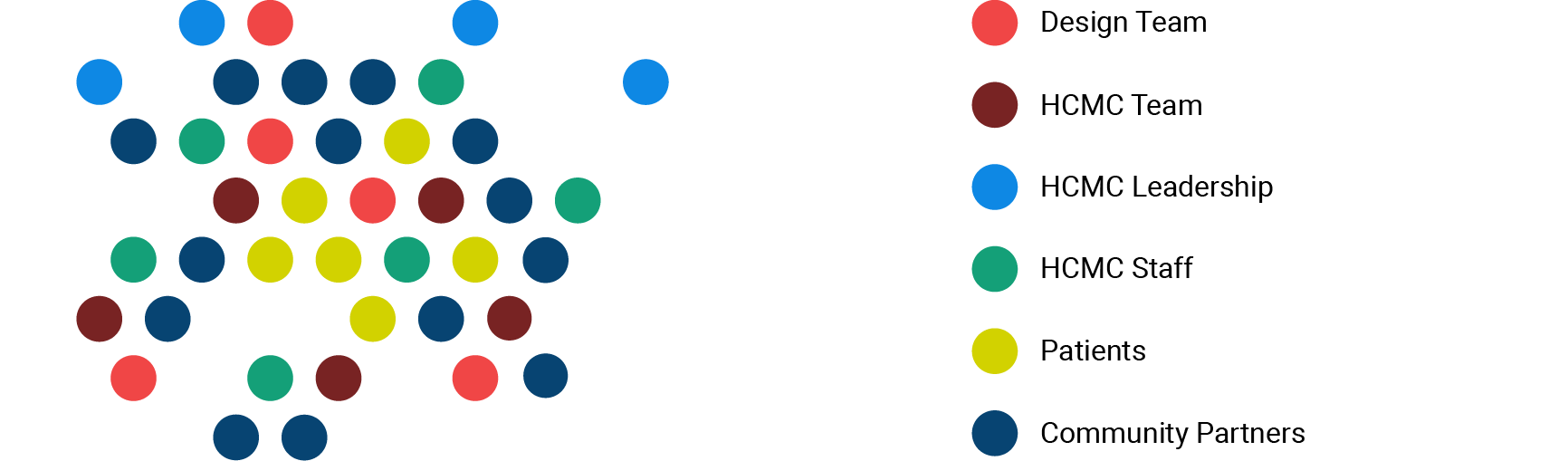
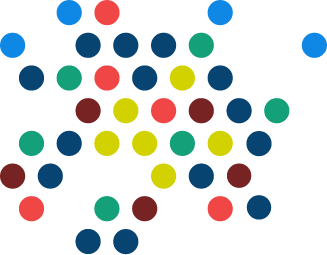
Team Structure and Dynamics
Geography and Reach
Client team (HCMC Upstream Innovations Team) – 5
Stakeholder team (HCMC leadership) – 15
Extended institutional team (HCMC staff) – 15
Patients engaged in research and prototyping – 20
Community partners (e.g. local nonprofit service providers) engaged in research and prototyping – 35
Total: 85 people
Objectives
Improve care for patients with complex conditions, who are more likely to face barriers in following their doctors’ orders.
Outcomes
A social enterprise called Hitch Health. hitchhealth.co was launched and built. The need for this concept was illuminated by the research. One of the 10 or 12 big concepts emerging from the ideation workshops was called Uber Health. HCMC found partners in Minneapolis and ran with that concept.
Largely anecdotal heightened awareness and interest in the HCD process that has not measured. Community partners lack the time/resources to do that.
“By leveraging HCD you are able to frame that problem correctly before moving forward. That was a big learning for me. We have been much more successful in creating services for the end user, our patient, with this process.” Susan Jepson, MPH, BSN, Vice President, Upstream Health Innovations, Hennepin County Medical Center
Client & Community Outcomes
Mindsets
By the end of the project, HCMC staff cultivated a deeper understanding of complex patients’ experiences and how to better support their needs on their journey towards healthier lives. After watching video of a patient traveling to and from her appointment, Patient Experience Officer Sheila Moroney shared, “This is the most I’ve learned about our patients in all the years I’ve worked at HCMC.”
Behaviors
Many concepts developed through this engagement were fast-tracked to implementation by HCMC’s team. One concept, Hitch Health, has already been spun out as a separate C Corporation, and is being offered to other safety net health systems. It’s a software product that seamlessly removes transportation barriers to and from the appointment, yielding powerful behavior change by decreasing clinic no-shows.
Culture
Our work coincided with the beginning of a culture shift at HCMC. The newly formed Upstream Health Innovations team had a mandate to shift the health system conversation towards a more proactive and holistic approach to health. Our work increased the organization’s understanding of the social determinants of health in communities, and opened the door to further collaboration with local community partners.
Resources
Tools
Greater Good Studio developed a concept called Priorities Conversation; a protocol of questions to aid medical assistants in engaging patients during the intake process. Its purpose was to help the care team understand a patient’s “big picture,” rather than only addressing their specific medical complaint. They worked with a primary care team to prototype and test this tool in a clinical setting. HCMC is continuing to iterate on the concept.
Programs
One program the design team developed, called Members Give Back, was meant to connect complex patients with work and volunteer opportunities. This concept was built off the insight that many patients desire to do more than take from society – they want to give back. They worked with a team at the HCMC day treatment center to prototype the program, in partnership with a local workforce development provider. The group built a curriculum and worked closely with 10 patients to help them build skills and find jobs. One year after the pilot, 100% of participants still had their jobs and/or were volunteering. The results have also shown a reduction in Emergency Department utilization and a decrease in inpatient stays.