MomConnect is an initiative of the National Department of Health (NDOH) supported by a range of partners in South Africa including Praekelt.org1. At the heart of the initiative is a national mobile messaging service that directly supports mothers, connects them to the health system and provides efficient access to health information for tracking and managing service delivery. Introduced in South Africa in 2014 as an SMS service, the MomConnect initiative now includes WhatsApp messaging, a health facility-based app to register pregnancies and a Road to Health app providing content around caring for children aged 0 – 5 years, developed by the MomConnect consortium of partners including Jembi Health Systems and Health Information Systems Program (HISP). MomConnect currently reaches 95% of public health facilities in South Africa and is available in 11 languages. The technology platform has also supported similar programs in Nigeria and Uganda.
This Case Study is focused on the design-approach that resulted in WhatsApp being introduced to MomConnect to deliver a cheaper and more impactful service text message service. But it is useful to first establish how design was approached in earlier in the MomConnect’s history.
MomConnect launched in 2014 as a USSD and SMS-based national pregnancy registry, through which every pregnant woman in South Africa could register to receive free, informative, stage-based messaging during pregnancy and for the first year (and up to two years from 2018) of her baby’s life. For users, the service provides access to a text-based Helpdesk where questions, complaints or compliments are sent directly to relevant officials to ensure mothers’ and nurses’ feedback drives service delivery improvements.
MomConnect was based on an earlier mobile health messaging program that developed content using funders’ materials and experience that was tailored to the South African clients and context, and tested with mothers for comprehension in different languages, as well as for comprehension and testing the tone of the messaging. Based on the caring personas of people who would normally give mothers advice, the developers created a composite persona to serve as the brand or voice of MomConnect. That voice is described as projecting a friendly tone as if receiving advice from a trusted source. “We were keen from a design perspective that the voice of MomConnect not be authoritative, but like a companion or friendly nurse.” Design in the form of user interviews and ethnography was also used to shape the service mothers received at health facilities including pregnancy registration and clinic processes.
The use of design in these early stages led the team to create a much bigger and impactful program. MomConnect was originally intended as data capture for pregnancy, introducing digital systems to facilitate data quality, flow and use. The team, applying the user-centered lens, went further to explore the acceptability of a new system with mothers and the nurses, asking: “What would make a mom want to sign up for this registration; What would make a nurse want to register a pregnancy on a mobile phone?” This was a fundamental change in how the project was viewed and in the approach taken by the MomConnect team. The idea of creating value for all the stakeholders in the ecosystem and motivating them to use MomConnect inspired the idea of making the program a mechanism for connecting mothers with the health system through their phones, providing health messages.
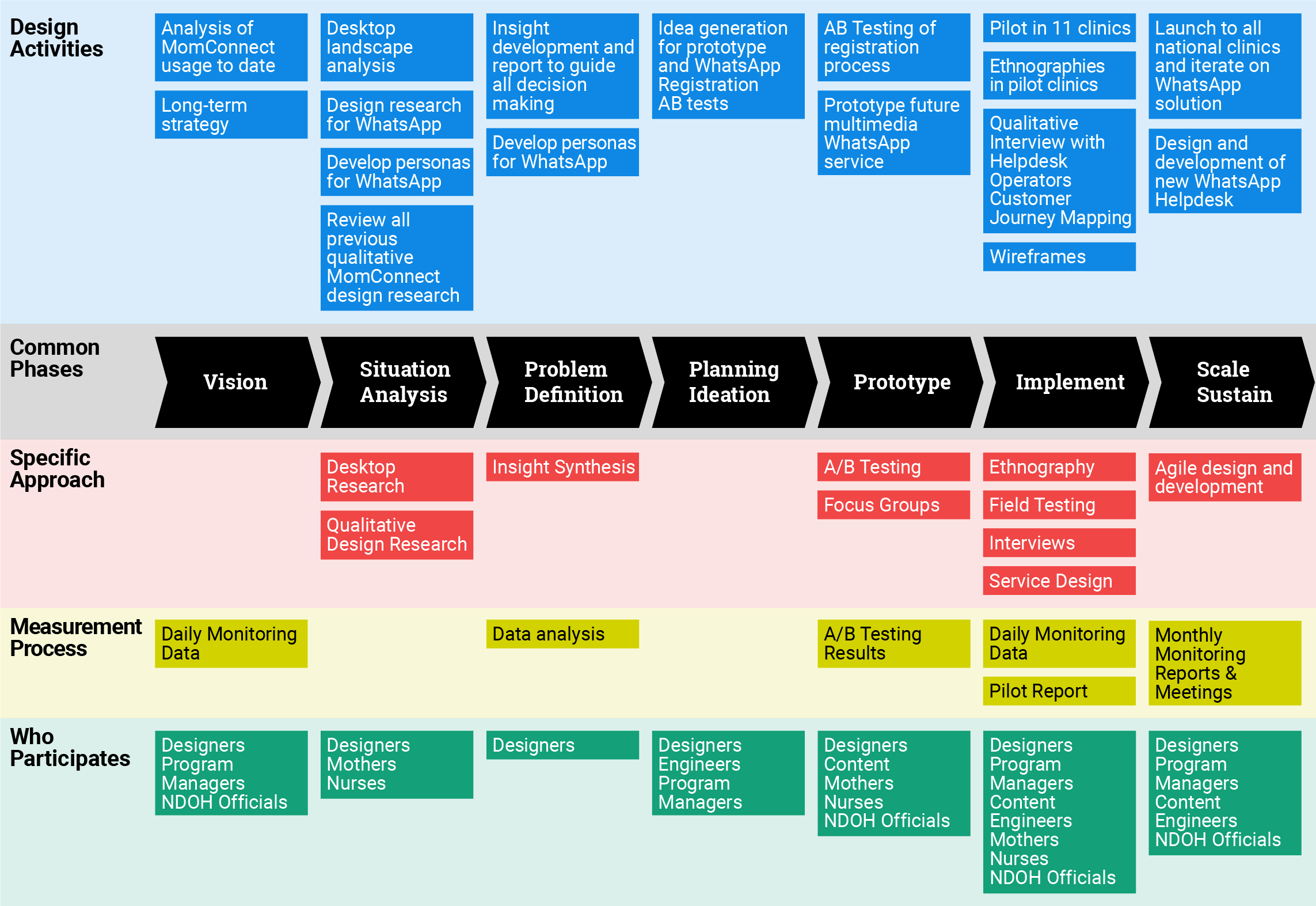
The mobile messaging uptake proved attractive to mothers. However, implementers felt that innovative efforts were essential but only if they could be delivered sustainably to every pregnant woman in the public health system in the country. For MomConnect, prohibitive SMS inventory costs to support the 800,000 women using MomConnect by 2017 threatened its sustainability. Sending essential information via SMS to pregnant women and new mothers was costing approximately USD 100,000 per month, over 40% of monthly program expenses, even after discounted rates were negotiated with local mobile network operators. To solve for this, MomConnect applied for and was chosen to be a WhatsApp development partner during the closed-group, beta development phase of their WhatsApp Business API. Through a rigorous service design process, they were able to understand the benefits of WhatsApp and design a simple solution for the mothers who want to use it, while ensuring they were still able to connect with the hardest to reach through SMS. Since the original design work (2017) that helped shape the next generation of MomConnect, the intervention has evolved even further. For example, the design research in 2017 resulted in a pilot with 394 mothers that tested a modified registration process to allow mothers to choose either WhatsApp or SMS. In April 2018, the USSD self-service option for switching from SMS to WhatsApp was introduced. A drive to encourage users to switch from SMS to WhatsApp was conducted in May 2018 and registration to WhatsApp as a default (if the user had an account) was introduced in September 2018.
1 Praekelt supported the DOH to develop a suite of mobile technologies, tools and methodologies that allow governments and other implementing partners to create and manage customize, population-scale health programs, like MomConnect.